Published: 10 December 2015
Publications
Statins - More Than Just Myopathy
Prescriber Update 36(4): 46-47
December 2015
Self-Limiting Myopathy and Rhabdomyolysis
Statins can cause myopathy that presents as muscle pain, tenderness, or weakness with or without raised levels of creatine kinase. Rhabdomyolysis is a more severe form of skeletal muscle damage that occurs with muscle related symptoms and creatine kinase levels greater than 10 times the upper limit of normal1.
These statin induced muscle effects are dose-dependent. Interactions of statins with CYP3A4 inhibitors may also increase exposure to statins. Therefore, it is important that the risks of myopathy and rhabdomyolysis are considered and managed when a statin is started or changed, during dose increases, and with the addition of any interacting medicines.
These direct myotoxic effects of statins are also referred to as "self-limiting" because symptoms tend to resolve either by lowering the dose, changing to a lower potency statin, or stopping the statin2.
Immune-Mediated Necrotising Myopathy
More recently, there have been reports of an immune-mediated necrotising myopathy associated with statin use. This autoimmune myopathy is characterised by progressive muscle weakness, elevated creatine kinase levels, and progression of signs and symptoms even when the statin is stopped3.
A comparison of self-limiting muscle effects and immune-mediated necrotising myopathy associated with statins is provided in Table 1.
Table 1: Comparison of self-limiting muscle effects and immune-mediated necrotising myopathy associated with statins4
| Self-limiting muscle effects | Immune-mediated necrotising myopathy | |
|---|---|---|
| Incidence | frequent | rare |
| Proximal weakness | infrequent | common |
| Creatine kinase levels | normal or mildly elevated, (>100,000 IU/L in rhabdomyolysis) |
elevated, 1000-50,000 IU/L |
| Timing relationship to statin | following initiation, resolve after discontinuation |
may present after years of usage; may appear or persist after statin discontinuation |
| Anti-HMG-CoA reductase antibody | absent | present |
| Electromyography | non-specific or normal | irritable myopathy |
| Biopsy | non-specific | prominent muscle necrosis with minimal or no inflammation |
| Treatment | statin withdrawal or dose reduction | statin withdrawal and immunosuppressive therapy |
An anti-HMG-CoA reductase autoantibody has been identified in association
with immune-mediated necrotising myopathies4.
Identifying this autoantibody in patients suspected to have statin-induced
necrotising autoimmune myopathy is useful to confirm the diagnosis4.
Treatment should include stopping the statin. Immunosuppressive therapy with agents such as prednisone, methotrexate, azathioprine, or ciclosporin may be required4.
New Zealand Reports
The Centre for Adverse Reactions Monitoring (CARM) has received 167 reports of self-limiting muscle effects associated with a statin during 2010 to 2014. These reports are summarised in Figure 1.
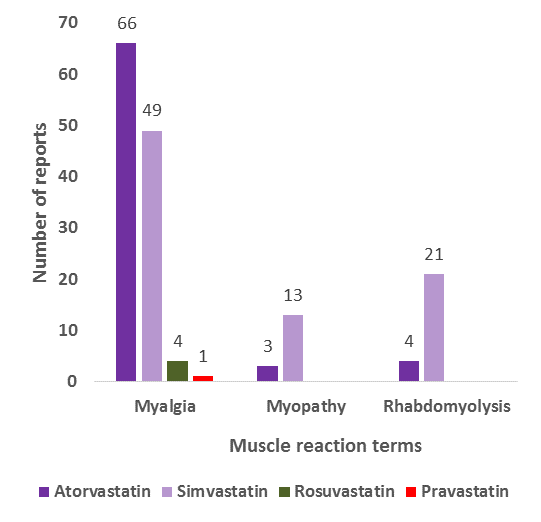
Figure 1: Reports to CARM of self-limiting muscle effects associated with a statin from 2010 to 2014
CARM has received one report of an immune-mediated necrotising myopathy associated with atorvastatin. This was reported to CARM in 2014.
Please continue to report any adverse reactions to statins, including muscle effects, to CARM. Reports can be submitted on paper or electronically (https://nzphvc.otago.ac.nz/).
References
- Sathasivam S, Lecky B. 2008. Statin induced myopathy. BMJ 337: a2286.
- Mohassel P, Mammen A. 2013. The spectrum of statin myopathy. Current Opinion in Rheumatology 25(6): 747-752.
- Merck Sharp & Dohme (New Zealand) Limited. 2014. Lipex Data Sheet 26 November 2014. URL: www.medsafe.govt.nz/profs/datasheet/l/Lipextab.pdf (accessed 23 October 2015).
- Babu S, Li Y. 2015. Statin induced necrotizing autoimmune myopathy. Journal of the Neurological Sciences 351: 13-17.


